
This article is based on ingredient functionality review, lab-scale formulation observations, and published skin-repair literature. It does not make clinical treatment claims. Finished-product performance and claims must be validated in the final formula.
Quick Answer: Is PDRN Good for Acne Scars?
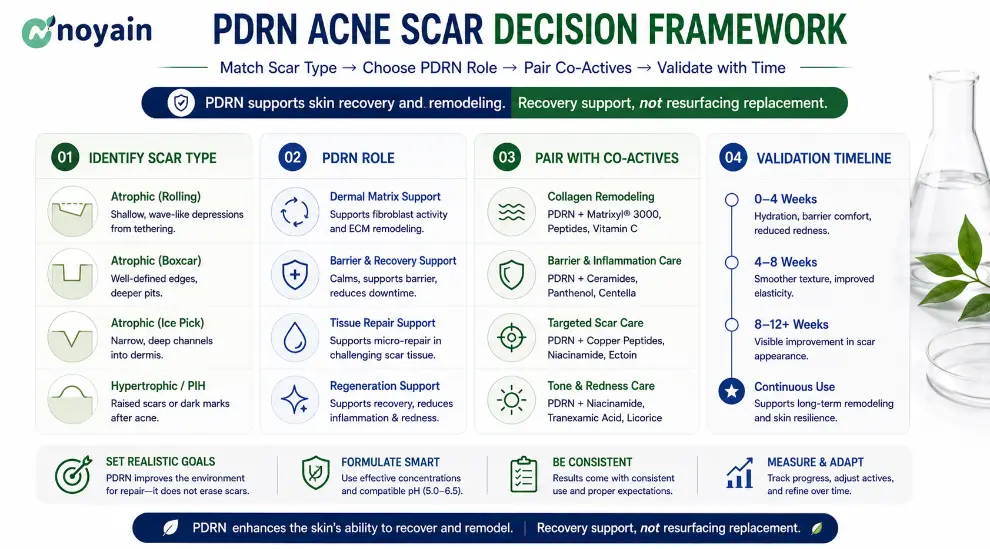
PDRN (INCI: Sodium DNA) is a useful recovery-support active for post-acne and acne-scar-positioned formulas, especially when the brief is sensitive skin, post-blemish redness, barrier recovery, or post-procedure support.
It should not be positioned as a stand-alone scar remover. For mature ice-pick, rolling, or boxcar scars, the realistic architecture is:
- PDRN serum or ampoule to support recovery, comfort, hydration, and repair signaling.
- A resurfacing strategy such as retinoids, azelaic acid, gentle exfoliation, microneedling, laser, or dermatology-led procedures when visible texture remodeling is the goal.
- A conservative claim window of 8-12 weeks for appearance, comfort, and smoothness perception, not “scar elimination.”
For the ingredient foundation, see our PDRN Complete Guide. For broader evidence, see PDRN Benefits for Skin.
Key Takeaways
- PDRN for acne scars is best positioned as post-blemish recovery support, not a resurfacing active.
- Acne-scar biology is inflammation-driven: atrophic scars are linked to collagen loss, matrix remodeling, and prolonged inflammatory signaling.
- PDRN’s most relevant pathways are adenosine A2A receptor activation and DNA salvage-pathway support.
- For topical cosmetic formulas, 0.3%-0.5% Sodium DNA is a practical starting range; going above 1.0% should be justified by claim value, not label storytelling.
- Add copper peptide to the compatibility table if you target
pdrn copper peptideandpdrn peptide serumsearches, but monitor color stability and metal-ion interactions. - Match the product format to the claim:
pdrn serum,pdrn ampoule,pdrn cream, and sheet mask concepts should not all use the same PDRN level. - Keep the FAQ tight. The article should answer the obvious questions in the body and reserve FAQ space for high-intent details.
The Formulation Problem: Acne Scars Are Not One Problem
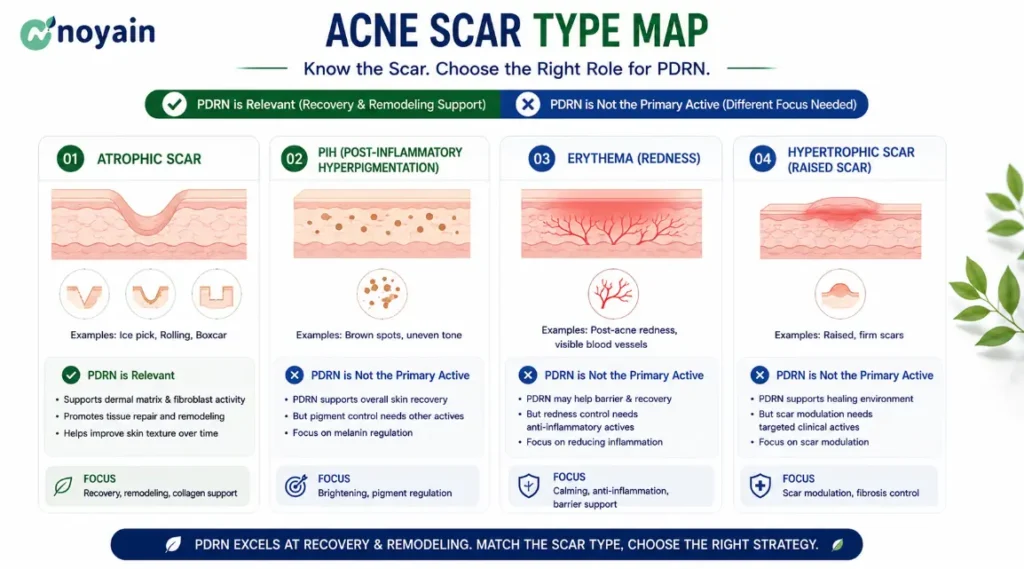
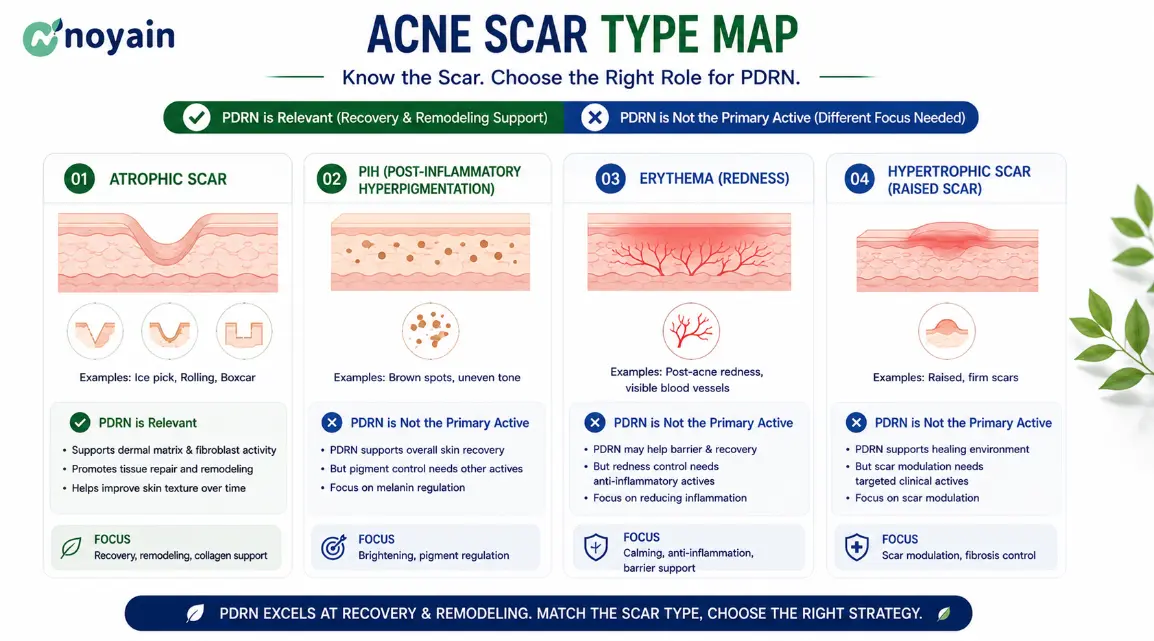
From a formulator’s perspective, “acne scars” usually blends several consumer concerns into one search query. The product architecture changes depending on which concern is real.
| Concern | Structural feature | What a topical formula can realistically support |
|---|---|---|
| Atrophic scars | Loss of collagen and elastic fiber structure | Recovery support + barrier repair + separate resurfacing strategy |
| Post-inflammatory erythema | Lingering redness after inflammation | Soothing + barrier repair + redness-control co-actives |
| Post-inflammatory hyperpigmentation | Melanin deposition without dermal tissue loss | Brightening actives + soothing support |
| Hypertrophic or keloid scars | Excess collagen deposition | Outside normal cosmetic leave-on scope; dermatology referral |
The distinction matters because most atrophic acne scars involve a net loss of dermal matrix, while PIH is mainly pigmentary. A PDRN product can help support a healthier recovery environment, but it cannot physically lift a mature deep scar by itself.
Acne-scar reviews commonly report that most acne scars are atrophic rather than hypertrophic. This is why a serious PDRN acne-scar formula should talk about collagen preservation, inflammation control, and recovery support, not only “glow” or “soothing.”
Why PDRN Is Different From Traditional Soothing Actives
Centella, panthenol, and madecassoside are valuable in post-acne formulas, but they do not tell the same mechanism story as PDRN.
| Active | Main mechanism | Scar-care relevance |
|---|---|---|
| Panthenol | Barrier repair and humectancy | Low to moderate |
| Centella extract | Soothing and redness support | Moderate |
| Madecassoside | Soothing + collagen-supportive positioning | Moderate |
| PDRN | A2A receptor signaling + nucleotide salvage support | High for recovery-support positioning |
| Retinoids | Cell turnover and collagen remodeling | High for texture, but irritation risk is higher |
Unlike centella or panthenol, PDRN is usually positioned as a regenerative-support active because it interacts with inflammatory signaling and nucleotide-recycling pathways. That does not make it stronger in every formula. It makes it different, and that difference is commercially useful when the product brief is premium post-blemish recovery.
How PDRN Works in Scar-Prone, Acne-Prone Skin
The mechanism is easiest to understand as a sequence:
mechanism -> scar biology -> formulation meaning
Why Inflammation Matters in Acne Scars
During inflammatory acne, neutrophils and macrophages release cytokines that activate matrix metalloproteinases (MMPs).
These enzymes degrade collagen and elastin around the follicle. Once enough extracellular matrix is lost, the skin can no longer rebuild the area completely, leading to rolling or boxcar scars.
From a formulation perspective, PDRN is interesting because it targets the inflammatory environment before collagen loss becomes difficult to reverse. That is the real formulation logic: not “PDRN fills the scar,” but “PDRN helps create a less inflammatory recovery environment.”
Pathway 1: Adenosine A2A Receptor Activation
PDRN is described in the pharmacology literature as an adenosine A2A receptor agonist. These receptors are present on fibroblasts, keratinocytes, endothelial cells, and immune cells.
In acne-prone skin, this matters because chronic low-grade inflammation after Cutibacterium acnes activity can keep the dermis in a tissue-remodeling state. That inflammatory loop is one reason matrix metalloproteinases (MMPs) become relevant: MMP activity is linked to collagen breakdown and abnormal extracellular-matrix remodeling.
Anti-inflammatory shift
This is where PDRN becomes useful to a formulator. The goal is to reduce the signals that keep post-acne skin hot, reactive, and matrix-degrading. In practical formulation language, that means:
- reducing the inflammatory noise that keeps post-acne skin reactive;
- supporting the M1-to-M2 macrophage polarization story used in repair biology;
- helping interrupt the cytokine/MMP cycle that can contribute to collagen degradation.
Formulation translation
PDRN is not “filling scars.” It is helping reduce the biological signals that keep damaged skin stuck in a low-grade inflammatory state. That is a more credible claim and a better memory point for formulators.
Fibroblast and collagen support
A2A activation is also linked to fibroblast activity, VEGF expression, angiogenesis support, and collagen-repair pathways. For atrophic acne scars, this is the relevant lever. It is also the reason PDRN fits better in a recovery-support system than in a fast resurfacing promise.
Data anchor
The 2020 cultured skin-cell study by Kim et al. found PDRN reduced MMP-1 activity/expression and melanin biosynthesis while supporting mitochondrial biogenesis. This is not a finished-product acne-scar clinical endpoint, but it gives formulators a concrete mechanistic bridge: MMP control + collagen-preservation logic + post-inflammatory discoloration support.
Pathway 2: DNA Salvage Pathway
PDRN also provides a pool of deoxyribonucleotide fragments that cells can reuse through the salvage pathway. In a recovery context, this is useful because stressed skin needs repair resources without the irritation burden of aggressive exfoliation.
For topical products, keep the caveat clear: standard PDRN serums do not deliver the same dermal exposure as injections or microneedling-assisted protocols. If your claim depends on deep dermal remodeling, build the product around procedure support or advanced delivery, not a basic water gel alone.
Should You Use PDRN for Acne Scars?
Atrophic acne scar or post-blemish texture concern?
|
+-- No -> Use pigment/redness/barrier strategy first.
|
+-- Yes
|
+-- Need recovery support after acne, peel, laser, or microneedling?
|
+-- Yes -> PDRN 0.3%-0.5% + niacinamide + panthenol
|
+-- No
|
+-- Sensitive or reactive skin?
|
+-- Yes -> PDRN + barrier actives; separate strong resurfacing.
|
+-- No -> Consider PDRN recovery serum + separate PM retinoid or azelaic acid.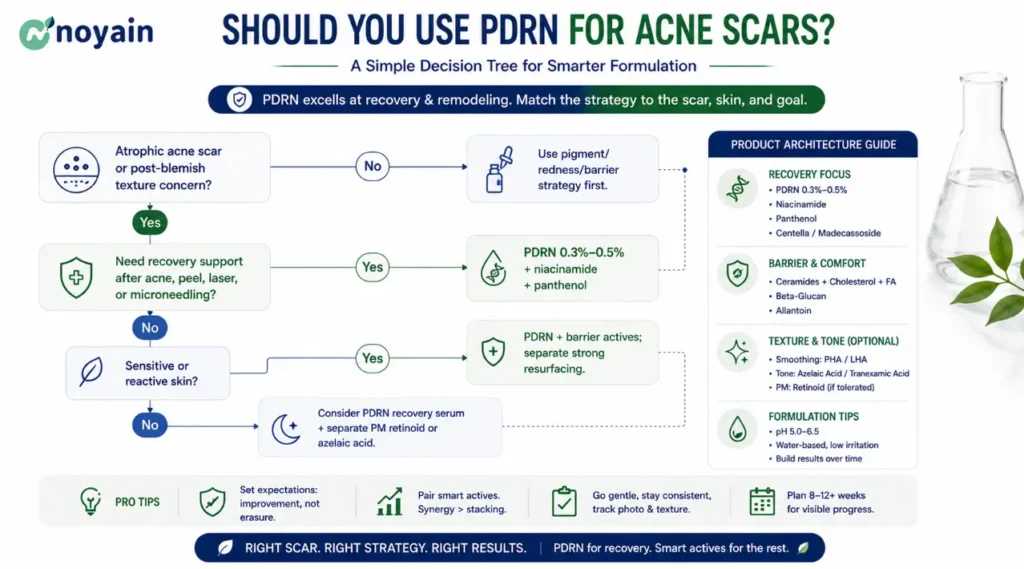
Which Product Format Makes Sense?
The best PDRN level depends on the format. A daily pdrn serum does not need the same use level or claim language as a premium pdrn ampoule, post-procedure sheet mask, or pdrn cream.
| Product format | Suggested PDRN level | Best positioning | Formulation note |
|---|---|---|---|
| Serum | 0.3%-0.5% | Daily recovery | Best fit for acne-prone skin, barrier comfort, and post-blemish routines |
| Ampoule | 0.5%-1.0% | Premium intensive recovery | Higher COGS can be justified if the claim and packaging support a premium story |
| Sheet mask | 0.2%-0.5% | Post-procedure comfort | Good fit after peel, laser, or microneedling support, but preservative and bioburden control matter |
| Cream | 0.1%-0.3% | Barrier support | Keep the chassis non-comedogenic and avoid heavy oils for acne-prone positioning |
For featured-snippet style clarity: use lower PDRN levels for daily barrier products, mid-range levels for serums, and higher levels only when the product format supports a premium recovery claim.
PDRN vs Microneedling for Acne Scars
This section targets high-intent comparison searches such as pdrn vs microneedling, pdrn acne scar treatment, and pdrn after microneedling.
| Approach | Speed | Downtime | Topical support role |
|---|---|---|---|
| PDRN serum | Slow | None | Excellent recovery-support active |
| Retinoid routine | Moderate | Mild irritation possible | Good if barrier is managed |
| Microneedling | Faster for texture | Several days | Benefits from recovery support |
| Laser resurfacing | Faster and stronger | Procedure-dependent | Benefits from post-procedure support |
The practical message is simple: PDRN should be viewed as recovery support, not a replacement for procedures. Microneedling creates controlled dermal injury to stimulate remodeling. PDRN fits naturally after that kind of intervention because the skin needs barrier comfort, redness support, and a repair-oriented environment.
Recent clinical procedure literature is starting to evaluate PDRN injections in acne-scar protocols. For example, a 2025 randomized, open-label study in Aesthetic Plastic Surgery compared air-botulinum toxin, PDRN, and their combination in 17 acne-scar participants; the combination arm showed the largest POSAS score reduction, while the PDRN-only arm also improved. This supports the direction of the recovery story, but it should not be used as proof that a standard topical serum can reproduce injectable outcomes.
Compatibility, Synergy, and Conflict
| Factor | What to check | Practical recommendation |
|---|---|---|
| pH | Final formula pH | Target pH 5.0-6.5. Avoid pH below 4.0 when PDRN is the headline active. |
| Solvent system | Water, glycols, ethanol | Prefer water + butylene glycol or pentylene glycol. Keep ethanol low; high-solvent systems rarely fit recovery-first acne-scar positioning. |
| Co-actives | Niacinamide, panthenol, allantoin, madecassoside, azelaic acid, retinoids | Niacinamide, panthenol, allantoin, and madecassoside are easy pairings. Use azelaic acid carefully with pH validation. Keep high-strength retinoids or strong acids in a separate routine step. |
| Copper peptide | Color, odor, metal-ion interactions | Compatible as a concept, especially for pdrn copper peptide and pdrn peptide serum positioning, but monitor color stability and complexation behavior. |
| Chelators | EDTA, sodium phytate, phytic acid | Use at the minimum functional level. Over-chelation can complicate metal-ion-sensitive systems and peptide pairings. |
| Processing | Temperature and shear | Add PDRN in water phase or cool-down below 40 C. Avoid prolonged high shear that may reduce fragment consistency. |
| Packaging | Airless pump, dropper, jar | Airless pump is preferred for a premium recovery serum. Droppers increase oxygen and user-contamination exposure. |
If you are choosing between PDRN and other active families, see our PDRN vs Retinol, Azelaic Acid & Exosomes comparison.
Example Formula: PDRN Post-Blemish Recovery Serum
This is a representative water-based serum chassis for an acne-prone, post-blemish, scar-supporting claim. It is a starting framework, not a finished product.
PDRN Post-Blemish Recovery Serum (illustrative)
Water (Aqua) ................................ q.s. to 100%
Butylene Glycol .............................. 6.00
Pentylene Glycol ............................. 3.00
Glycerin ..................................... 4.00
Sodium DNA (PDRN) ............................ 0.50
Niacinamide .................................. 3.00
Panthenol .................................... 2.00
Allantoin .................................... 0.30
Madecassoside ................................ 0.20
Centella Asiatica Extract .................... 1.00
Hydroxyethylcellulose ........................ 0.40
Phenoxyethanol, Ethylhexylglycerin ........... 1.00
Disodium EDTA ................................ 0.05-0.10
pH adjuster ................................. q.s. to pH 5.5 +/- 0.3Formulator’s Note
Why 0.5% PDRN? It is a defensible mid-range starting point. Going above 1.0% often increases COGS faster than sensory or perceived performance gains.
Why 3% niacinamide instead of 10%? Post-acne skin is often reactive. A moderate level supports tone and barrier positioning without pushing irritation risk too hard.
Why no ethanol? High-solvent systems rarely fit the recovery-first positioning of acne-scar products.
Why no strong acid in the same bottle? If texture remodeling is the goal, use a separate PM resurfacing step. Let the PDRN product own recovery, comfort, and barrier support.
Bench Observation
In our experience, PDRN itself rarely causes stability problems.
Most failures come from:
- botanical extract discoloration;
- excessive glycerin causing tackiness;
- broad molecular-weight distribution between lots;
- overuse of chelators;
- copper-peptide combinations without color screening.
Ironically, the “PDRN problem” is often not a PDRN problem at all. It is usually a chassis, supplier-specification, or co-active compatibility problem.
Troubleshooting Before Scale-Up
| Problem | Possible cause | What to try |
|---|---|---|
| Serum yellows over 4 weeks | Botanical extract oxidation, peptide interaction, or low-purity DNA material | Tighten packaging, reduce extract load, check color stability with and without copper peptide, request higher-purity PDRN grade |
| Viscosity drops at 8 weeks | Thickener instability in glycol-rich system | Screen alternate thickeners and confirm pH drift at 25 C and 40 C |
| Sticky sensory | Humectant load too high or PDRN grade too high-MW | Rebalance glycerin/glycol ratio and request a defined molecular-weight band |
| Patchy redness in use test | Vehicle irritation rather than PDRN | Audit fragrance, ethanol, essential oils, low pH, and strong acid carryover |
| No visible texture change | PDRN was expected to replace resurfacing | Reposition as recovery support and add separate retinoid, azelaic acid, peel, or procedure pathway |
When PDRN Will Probably Disappoint
PDRN is unlikely to deliver meaningful visible changes when:
- ice-pick scars are already mature and deeply fibrotic;
- consumers expect structural remodeling within four weeks;
- the formula relies on PDRN alone without any resurfacing or procedure strategy;
- high-irritation actives compromise barrier recovery;
- the raw material is poorly characterized and the active PDRN load is unclear.
In these cases, procedures such as microneedling, laser resurfacing, subcision, or combination routines are usually more realistic approaches. PDRN can still play a role, but it is the recovery-support layer, not the entire treatment plan.
Validation Timeline
Before claiming “post-acne recovery” or “scar-support” benefits, run a minimum 0w / 4w / 8w / 12w stability and sensory program.
| Time point | Test items |
|---|---|
| 0w release | Appearance, color, odor, pH, viscosity, specific gravity, microbial limits, sensory baseline |
| 4w | pH drift, viscosity drift, color/odor shift, centrifugal stability, early packaging check |
| 8w | Sensory re-evaluation, phase stability, accelerated stability pull, packaging compatibility |
| 12w | Final stability review at 25 C, 30 C, and 40 C; preservative challenge test result; claim sign-off |
Acceptance criteria we use with brand teams
- pH drift within +/- 0.3 from release.
- Viscosity drift within +/- 15% from release.
- No visible color shift beyond the approved reference standard.
- PCT pass at 28 days.
- No phase separation at any checkpoint.
What We Consider a Failed Prototype
We usually reject a prototype when:
- pH drift exceeds +/- 0.3;
- viscosity changes by more than 15%;
- noticeable yellowing appears after 8 weeks;
- consumer sensory scores drop below the initial panel average;
- the formula needs a higher PDRN level to compensate for a weak chassis.
A stable formula is more valuable than adding another 0.2% PDRN.
Supplier Red Flag
If a supplier cannot clearly define the assay on dry basis, molecular-weight distribution, endotoxin specification, and batch-to-batch consistency, the quoted PDRN percentage on the brochure means very little.
Always request:
- assay on dry basis;
- molecular-weight distribution;
- endotoxin level;
- batch-to-batch consistency data;
- BSE/TSE declaration;
- COA, TDS, SDS, MOQ, lead time, and lot-to-lot consistency data.
Two “0.5% PDRN” materials may perform completely differently if one has a broad molecular-weight distribution and the other has a controlled fragment band.
If you want a direct conversation on PDRN grade, molecular-weight band, or sample availability for an acne-scar or post-blemish concept, our Sodium DNA product page lists the standard documentation and contact route.
FAQ
Is PDRN safe for acne-prone skin?
PDRN itself is usually well tolerated at typical cosmetic use levels, but the vehicle matters more than the active. Avoid heavy comedogenic oils, high ethanol, strong fragrance, and unnecessarily low pH in acne-prone formulas.
What percentage of PDRN should I use for a post-acne serum?
For leave-on serums and ampoules, 0.3%-0.5% Sodium DNA is a practical starting range. Up to around 1.0% can be considered for premium recovery masks or post-procedure products, but the claim value should justify the COGS.
Can PDRN be used with retinol or azelaic acid?
Yes, but the cleanest architecture is often a separate recovery product and a separate resurfacing product. PDRN pairs more comfortably with azelaic acid at modest levels than with high-strength retinoids or high-percentage AHA/BHA in the same bottle.
Does PDRN help active acne or only post-acne marks?
In cosmetics, PDRN is better positioned for post-acne recovery, barrier support, redness comfort, and scar-support routines. Active moderate-to-severe acne should be handled with appropriate acne actives and dermatology guidance.
How long does PDRN take to show results on acne-scarred skin?
For a topical cosmetic formula, use an 8-12 week claim window for smoothness perception, comfort, hydration, and recovery support. Mature atrophic scars usually need a resurfacing or procedure-based strategy for visible structural change.
References
- Squadrito F., Bitto A., Irrera N., Pizzino G., Pallio G., Minutoli L., Altavilla D. Pharmacological Activity and Clinical Use of PDRN. Frontiers in Pharmacology, 2017. DOI: 10.3389/fphar.2017.00224.
- Colangelo M.T., Galli C., Guizzardi S. Polydeoxyribonucleotide Regulation of Inflammation. Advances in Wound Care, 2020. DOI: 10.1089/wound.2019.1031.
- Kim Y.J., Kim M.J., Kweon D.K., Lim S.T., Lee S.J. Polydeoxyribonucleotide Activates Mitochondrial Biogenesis but Reduces MMP-1 Activity and Melanin Biosynthesis in Cultured Skin Cells. Applied Biochemistry and Biotechnology, 2020. DOI: 10.1007/s12010-019-03171-2.
- Connolly D., Vu H.L., Mariwalla K., Saedi N. Acne Scarring: Pathogenesis, Evaluation, and Treatment Options. Journal of Clinical and Aesthetic Dermatology, 2017.
- Sitohang I.B.S., Sirait S.A.P., Suryanegara J. Microneedling in the Treatment of Atrophic Scars: A Systematic Review of Randomised Controlled Trials. International Wound Journal, 2021. DOI: 10.1111/iwj.13559.
- Park M.H., Hwang S.K., Hwang J.K., Chua D., Yi K.H. Air-Botulinum Neurotoxin and Polydeoxyribonucleotide Injections for Acne Scar Treatment. Aesthetic Plastic Surgery, 2025. DOI: 10.1007/s00266-025-05157-4.
- EU CosIng database, entry for Sodium DNA (INCI).
{kind=link}
{kind=link}
{kind=link}